EURO-CTO
Brief summary
CTOs are common among patients with angina, and are detected in around 20% of patients undergoing coronary angiography. Treatment of CTO has been found to constitute only 7% of PCI practice on average. One of the reasons for the under-presentation of CTOs in PCI target lesions is the lack of evidence-based medical data on treatment indications, and the continued low level of accepted evidence for the treatment of CTOs by PCI in PCI guidelines.
Patients with a CTO represent patients with stable coronary artery disease. The COURAGE trial comparing PCI with optimal medical therapy in stable coronary disease did not show a difference in mortality or myocardial infarction between the two treatment options. However, CTOs were not included in the COURAGE trial. But that trial did confirm the superiority of PCI over OMT in controlling symptoms of angina, with a high cross-over rate to PCI. Whether PCI for CTO is superior to OMT in reducing MACE in those patients with a large ischaemic burden has never been tested in a randomized controlled trial.
While there is compelling evidence from registry studies of a clinical and prognostic benefit following successful PCI of CTO compared with PCI failure, there has been no randomized controlled trial of contemporary PCI using drug-eluting stents versus optimal medical therapy. The COURAGE trial nuclear sub-study confirms both that prognosis is closely related to the extent of residual ischaemia and that PCI is more effective in reducing residual ischaemia than optimal medical therapy alone. This confirms earlier retrospective data suggesting that the benefit of PCI is greatest in patients with moderate (10-20%) or severe (>20%) ischaemia.
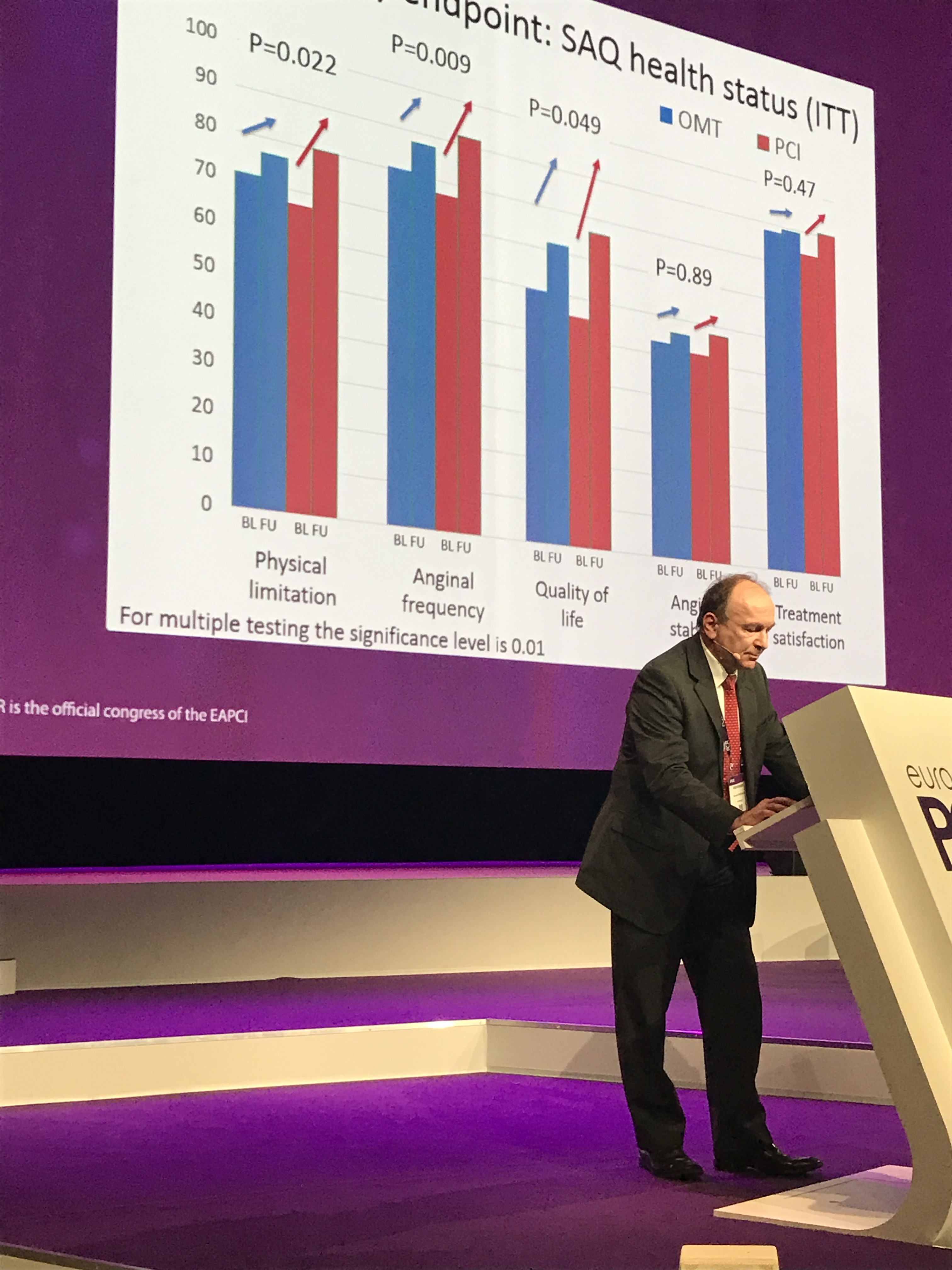
Study hypothesis: PCI with Biolimus eluting stent implantation plus OMT will be superior to OMT alone in improving health status at 12-month follow-up, and will be noninferior with respect to the composite of all cause death/ non fatal MI at 36-month follow up, in patients with a CTO in an epicardial coronary artery >2.5 mm diameter and chronic stable angina with evidence of ischemia and viability in the territory subtended by the CTO
Primary endpoints
-
- Quality of Life [ Time Frame: Baseline and 12 months : Seattle Angina Questionnaire and EQ-5D for health outcomes measurement
- Major cardiovascular events [ Time Frame: 36 months]:Cumulative composite endpoint of all-cause death, non-fatal MI at 3 years
CERC Services
- Full service
Countries
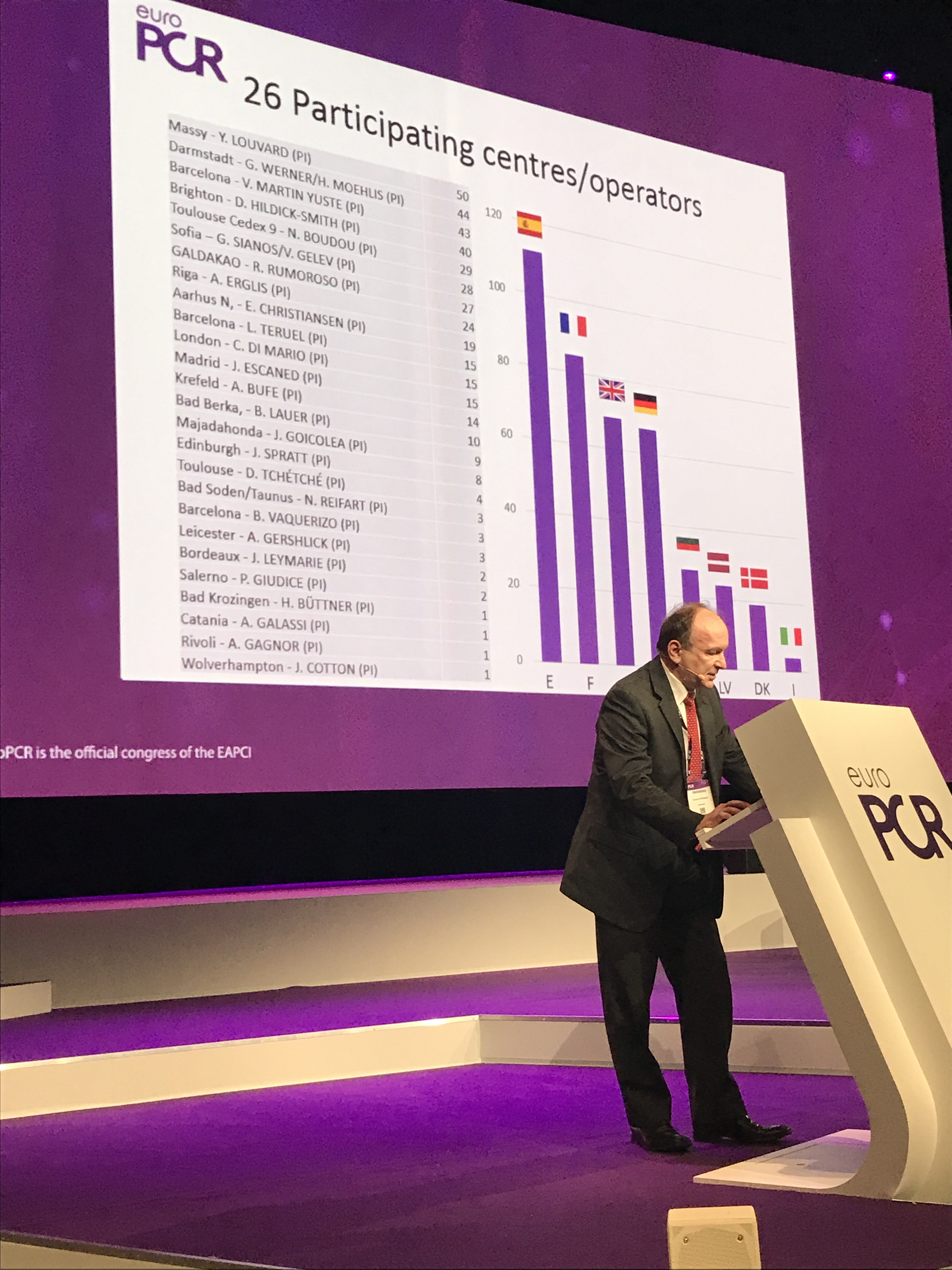
France, Germany, UK, Spain, Latvia, Bulgaria, Denmark, Italy, Sweden
Centers number
30 centers managed by CERC.
EuroPCR 2017: